Use of CBCT in Endodontic Treatment Planning with Impacted Wisdom Teeth

CBCT findings are sometimes surprising. Below are three cases where radiographic findings related to impacted wisdom teeth changed the treatment plan. Keep in mind that the radiation exposure from the Kodak 9000 3D for each of these cases is reported by Kodak to be similar to four standard periapical radiographs.
Case #1: You Better Keep that Tooth
This patient presented with a referral slip for tooth #3 saying “Evaluate restorability and treat if necessary.” The deep distal decay on #3 presented a generally unfavorable long-term prognosis without crown lengthening. Treatment options included endodontic treatment of #3, build-up, and crown; extraction of #3 and placement of a bridge from #2 – #4; or extraction and implant of #3. A CBCT was taken to evaluate the true relationship of the decay to the crestal bone. A surprise finding was that the impacted wisdom tooth had caused an area of resorption on the distal buccal and palatal root of #2.
Because of the CBCT findings, we could determine that #2 was not restorable. With the removal of #2, adequate access to the distal of #3 can be made for a more predictable and favorable restoration. Had the CBCT not been taken, and if the patient had decided to remove #3 in favor of a bridge, she would have eventually lost #2 as well. CBCT imaging thus saved the patient the cost of a bridge and the unnecessary removal of tooth #3. Although the argument for an implant in this case could be made, a favorable long-term prognosis is expected with endodontic treatment and restorative. Further evaluation of the impacted #32 still needs to be performed and is suggested. (Click thumbnails below for full images)


Case #2: You Better Lose that Tooth
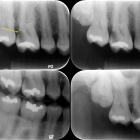
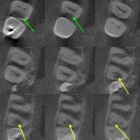
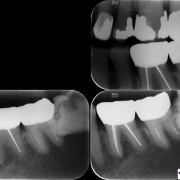
This patient presented having discussed options with his dentist on whether he should keep or remove tooth #2. The bitewing radiograph demonstrates that the tooth is in limited function. Periapical radiographs show that tooth #1 is in close proximity, but that the relationship is relatively benign. Despite the limited value of this tooth, the patient opted to keep it through endodontic treatment and a crown.
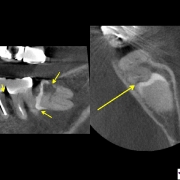
CBCT imaging revealed that the cusps of tooth #1 are driving into the palatal root of tooth #2. Although the damage appears to be minimal, I could not guarantee the long-term favorability of this tooth given the already present damage to the palatal root. The findings from the CBCT added the final piece of evidence to suggest a less than favorable long-term result, and the patient opted for removal of the tooth. Once again, the CBCT findings offered information that saved the patient the unnecessary expense of endodontic and restorative treatment.

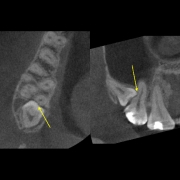
Case #3: Your Problem is a Different Tooth
This frail 87 year old female patient presented with pain in the lower left side. She was referred for possible re-treatment of tooth #19 silver points due to vague symptoms of a dull ache on the lower left side. Whereas standard radiographs suggested a problem with tooth #17, CBCT imaging confirmed an irregular radiographic finding consistent with decay. Our ultimate diagnosis was an irreversible pulpitis of the impacted tooth #17, and she was referred to an oral surgeon for evaluation and removal. In this case the CBCT provided information that allowed for proper treatment planning and discussion of the possible loss of #18 due to the proximity of the wisdom tooth. Standard radiographs provided information about the integrity of the distal margin of #19, which was also discussed.
We learn at least two things from theses three cases. 1) Impacted third molars can cause damage to adjacent teeth and should be removed at an early age when morbidity is low. Although many potential complications were present with removing the wisdom tooth on the 87 year old female, reports from the oral surgeon suggested a successful outcome. 2) Use of the CBCT, even when you think you have all the information you need with standard radiographs, provides treatment planning information that suggest endodontic treatment is needed, that endodontic treatment is not needed, or a different treatment is necessary. These ultimately offer value to the patient with proper treatment planning leading to improved longevity of dental treatment.
Good stuff? Maybe pass it along!
Other Recent Posts:
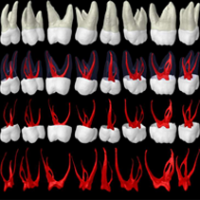
Root Canal Anatomy is Complex
By Dr. Peter Shelley
What do Shoelaces and Sutures Have in Common?
By Dr. Peter Shelley